Ureteral Obstruction
Overview
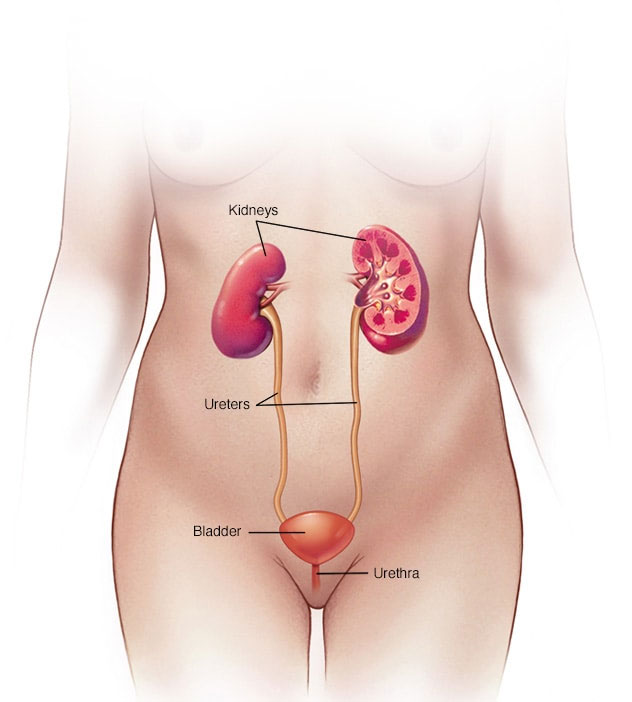
Female urinary system
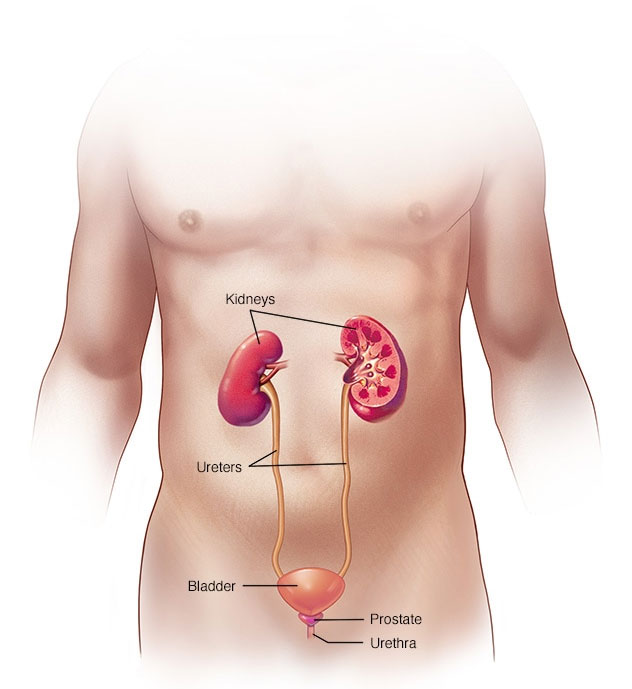
Male urinary system
Laparoscopic Approach
Laparoscopic pyeloplasty is a way to perform reconstructive surgery of a narrowing or scarring where the ureter (the tube that drains urine from the kidney to the bladder) attaches to the kidney through a minimally invasive procedure.
This operation is used to correct a blockage or narrowing of the ureter where it leaves the kidney. This abnormality is called a ureteropelvic junction (UPJ) obstruction which results in poor and sluggish drainage of urine from the kidney. UPJ obstruction can potentially cause abdominal and flank pain, stones, infection, high blood pressure and deterioration of kidney function.
When compared to the conventional open surgical technique, laparoscopic pyeloplasty has resulted in significantly less post-operative pain, a shorter hospital stay, earlier return to work and daily activities, a more favorable cosmetic result and outcomes identical to that of the open procedure.
The Surgery
Ureteropelvic Junction (UPJ) Obstruction
Laparoscopic pyeloplasty is performed under general anesthesia. The typical length of the operation is three to four hours. The surgery is performed through three small (1 cm) incisions made in the abdomen. A telescope and small instruments are inserted into the abdomen through these keyhole incisions, which allow the surgeon to repair the blockage/narrowing without having to place his or her hands into the abdomen.
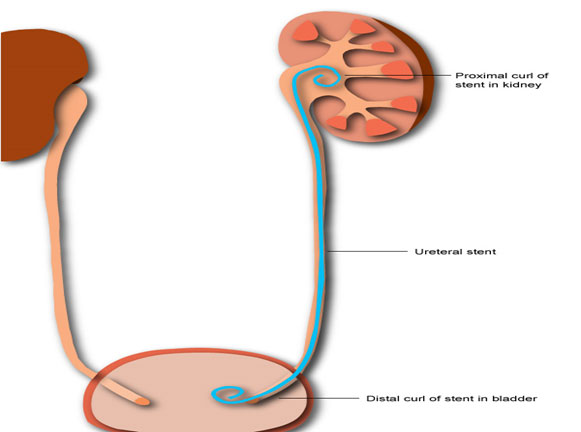
A small plastic tube (called a ureteral stent) is left inside the ureter at the end of the procedure to bridge the pyeloplasty repair and help drain the kidney. This stent will remain in place for four weeks and is usually removed in the doctor's office. A small drain will also be left exiting your flank to drain away any fluid around the kidney and pyeloplasty repair.
Potential Risks & Complications
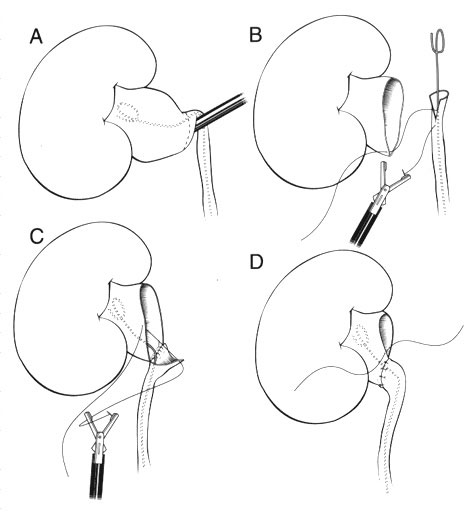
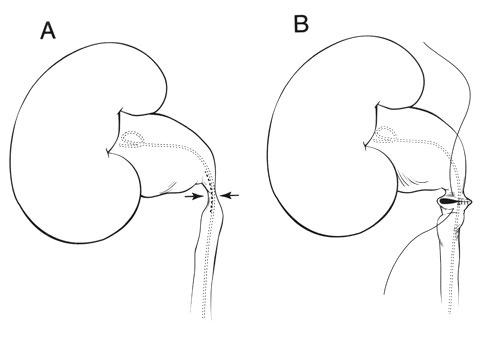
Laparoscopic dismembered pyeloplasty
Although this procedure has proven to be very safe, as in any surgical procedure there are risks and potential complications. The safety and complication rates are similar when compared to the open surgery. Potential risks include:
-
Bleeding: Blood loss during this procedure is typically minor (less than 100 cc) and a blood transfusion is rarely required. If you are still interested in autologous blood transfusion (donating your own blood) prior to your surgery, you must make your surgeon aware. When the packet of information is mailed or given to you regarding your surgery, you will receive an authorization form for you to take to the Red Cross in your area.
-
Infection: All patients are treated with broad-spectrum intravenous antibiotics prior to starting the surgery to decrease the chance of infection from occurring after surgery. If you develop any signs or symptoms of infection after the surgery (fever, drainage from your incision, urinary frequency, discomfort, pain or anything that you may be concerned about) please contact us at once.
-
Hernia: Hernias at incision sites rarely occur since all keyhole incisions are closed carefully at the completion of your surgery.
-
Tissue / organ injury: Although uncommon, possible injury to surrounding tissue and organs including bowel, vascular structures, spleen, liver, pancreas and gallbladder could require further surgery. Injury could occur to nerves or muscles related to positioning.
-
Conversion to open surgery: this surgical procedure may require conversion to the standard open operation if extreme difficulty is encountered during the laparoscopic procedure. This could result in a larger standard open incision and possibly a longer recuperation period.
-
Failure to correct UPJ obstruction: Roughly 3% of patients undergoing this operation will have persistent blockage due to recurrent scarring. If this occurs additional surgery may be necessary.
A ureteral obstruction is a blockage in one or both of the tubes (ureters) that carry urine from the kidneys to the bladder. Ureteral obstruction can be cured. However, if it's not treated, symptoms can quickly move from mild — pain, fever and infection — to severe — loss of kidney function, sepsis and death.
Ureteral obstruction is fairly common. Because it's treatable, severe complications are rare.
Symptoms
Ureteral obstruction might have no signs or symptoms. Signs and symptoms depend on where the obstruction occurs, whether it's partial or complete, how quickly it develops, and whether it affects one or both kidneys.
Signs and symptoms might include:
-
Pain
-
Changes in how much urine you produce (urine output)
-
Difficulty urinating
-
Blood in the urine
-
Urinary tract infections
-
High blood pressure (hypertension)
Causes
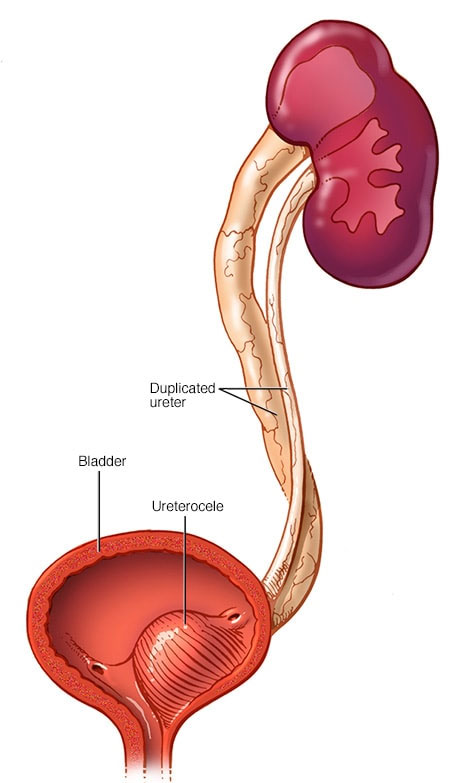
Duplicated ureter and ureterocele
Different types of ureteral obstruction have different causes, some of them present at birth (congenital). They include:
-
A second (duplicated) ureter.This common condition, which is congenital, causes two ureters to form on the same kidney. The second ureter can be fully or only partially developed. If either ureter doesn't work properly, urine can back up into the kidney and cause damage.
-
A blockage (obstruction) where the ureter connects to the kidney or bladder.This prevents urine flow. A blockage where the ureter and kidney meet (ureteropelvic junction) may cause the kidney to swell and eventually stop working. This condition can be congenital or can develop with typical childhood growth, result from an injury or scarring, or in rare cases, develop from a tumor. A blockage where the ureter and bladder meet (ureterovesical junction) may cause urine to back up into the kidneys.
-
If a ureter is too narrow and doesn't allow urine to flow completely, a tiny bulge in the ureter (ureterocele) may develop. When a ureterocele develops, it's usually in the section of the ureter closest to the bladder. This can block urine flow and cause urine to back up into the kidney, possibly leading to kidney damage.
-
Retroperitoneal fibrosis.This rare disorder occurs when fibrous tissue grows in the area behind the abdomen. The fibers may grow as the result of cancer tumors or from taking certain medicines used to treat migraines. The fibers encircle and block the ureters, causing urine to back up into the kidneys.
Other possible causes
Various causes inside (intrinsic) or outside (extrinsic) the ureter can lead to ureteral obstruction, including:
-
Kidney stones
-
Cancerous and noncancerous tumors
-
Blood clots
-
Enlarged lymph nodes
-
Internal tissue growth, such as endometriosis in females
-
Long-term swelling of the ureter wall, usually due to diseases such as tuberculosis or a parasite infection called schistosomiasis
Complications
Ureteral obstruction can lead to urinary tract infections and kidney damage, which can be irreversible.
Diagnosis
Often, providers diagnose ureteral obstruction disorders before birth during routine prenatal ultrasounds, which can show details of the developing fetus, including the kidneys, ureters and bladder. Providers often perform another ultrasound after birth to reevaluate the kidneys.
If your provider suspects you have an obstructed ureter, some of these tests and scans might be used to reach a diagnosis:
-
Blood and urine tests.Your provider checks samples of your blood and urine for signs of infection and the presence of creatinine, which signals that your kidneys aren't working properly.
-
An ultrasound of the area behind your abdominal organs (retroperitoneal ultrasound) allows your provider to view the kidneys and ureters.
-
Bladder catheterization.To test for incomplete or blocked urine flow, your provider inserts a small tube (catheter) through the urethra, injects dye into your bladder, and takes X-rays of your kidneys, ureters, bladder and urethra before and during urination.
-
Renal nuclear scan.Your provider or a technician injects a tracer that contains a small amount of radioactive material into your arm. A special camera detects the radioactivity and produces images that your provider uses to evaluate the urinary system.
-
A small tube with a camera and light is inserted into your urethra or through a small incision. The optical system allows the provider to see inside the urethra and bladder.
-
Computerized tomography (CT) scan.A CT scan combines a series of X-ray views taken from many different angles and computer processing to create cross-sectional images of your kidneys, ureter and bladder.
-
Magnetic resonance imaging (MRI).An abdominal MRI uses a magnetic field and radio waves to create detailed images of the organs and tissues that make up your urinary system.
Treatment
The goal of ureteral obstruction treatment is to remove blockages, if possible, or bypass the blockage, which may help repair damage to the kidneys. Treatment might include antibiotics to clear associated infections.
Drainage procedures
A ureteral obstruction that causes severe pain might require an immediate procedure to remove urine from your body and temporarily relieve the problems caused by a blockage. Your doctor (urologist) may recommend:
-
A ureteral stent,which is a hollow tube inserted inside the ureter to keep it open.
-
Percutaneous nephrostomy,during which your doctor inserts a tube through your back to drain the kidney directly (percutaneous nephrostomy).
-
A catheter,which is a tube inserted through the urethra to connect the bladder to an external drainage bag. This may be especially important if problems with your bladder also contribute to poor drainage of your kidneys.
Your doctor can tell you which procedure or combination of procedures is best for you. Drainage procedures might provide temporary or permanent relief, depending on your condition.
Surgical procedures
There are a number of surgical procedures used to correct ureteral obstructions. The type of procedure depends on your situation.
Ureteral obstruction surgery may be performed through one of these surgical approaches:
-
Endoscopic surgery.This minimally invasive procedure involves passing a lighted scope through the urethra into the bladder and other parts of the urinary tract. The surgeon makes a cut into the damaged or blocked part of the ureter to widen the area and then places a hollow tube (stent) in the ureter to keep it open. This procedure may be done to both diagnose and treat a condition.
-
Open surgery.The surgeon makes an incision in your abdomen to remove the blockage and repair your ureter.
-
Laparoscopic surgery.In this approach, the surgeon makes one or more small incisions through your skin to insert a small tube with a light, a camera and other instruments needed for the procedure.
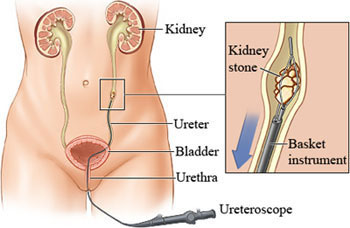
Ureteral Stone Treatment
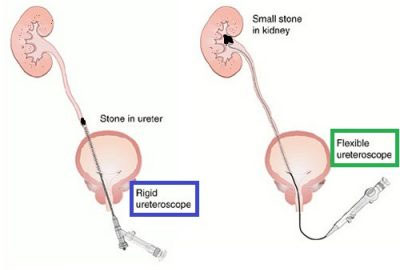
Endoscopic Ureteric surgery
Flexible or digital ureteroscope which has very narrow diameter is introduced into the ureter via the urethra (without anu external incision) and the stone is accessed and fragmented using lithotripter or laser as is appropriate according to case.
In few cases due to the stone there is swelling and the efforts to remove the stone can lead to injury to ureter. In these cases stent is introduced and after a few weeks as the tract is dilated and the selling decreases the procedure is completed.